BACTERIAL MENINGITIS Timeline, Organisms, Presentation

BACTERIAL MENINGITIS Timeline, Organisms, Presentation
More Posts from T-b-a-blr-blog and Others

(Day 4/100 days of productivity) - Haemophilus Influenzae card!
Today was mostly spent working on research, textbooks, but and making flashcards like this for microbiology!
Pneumonia
“Pneumonia is called the old man’s friend because, left untreated, the sufferer often lapses into a state of reduced consciousness, slipping peacefully away in their sleep, giving a dignified end to a period of often considerable suffering.” -Dr John Pillinger
Pneumonia is a major cause of morbidity and mortality worldwide, the 6th largest cause of death in the USA. It is also economically costly in antibiotics, time off work, and hospitalisation
In half the cases the cause is not identified
In those where a cause is identified, S. pneumoniae is the most common cause
The reservoir is usually humans (oneself or a contact)
spread is through respiratory droplets
Community acquired eg Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Mycoplasma pneumoniae, Chlamydia pneumoniae
Noscomial (hospital acquired) eg Enterobacteriaceae, Staphylococcus aureus, Anaerobes, Pseudomonas aeruginosa
Many patients have an underlying condition, e.g. bronchitis, asthma, a viral infection, tumours
Characterised by the alveolar sacs filling up with pus, giving rise to a purulent sputum
Symptoms
Results in chest tightness or pain, difficulty in breathing, fever or hypothermia, reduced blood oxygen, coughing to clear mucus, chest will sound “dull” when tapped, tachypnea, tachycardia (>100 bpm) or bradycardia (< 60 bpm), central cyanosis, altered mental status.

Streptococcus pneumoniae: Rust-colored sputum
Pseudomonas, Haemophilus, and pneumococcal species: May produce green sputum
Klebsiella species pneumonia: Red currant-jelly sputum
Anaerobic infections: Often produce foul-smelling or bad-tasting sputum
Diagnosis
X-ray showing infiltrates
Elevated temperature
Changes in WBC counts
Culture confirmation
Serum chemistry panel
Arterial/venous blood gas
Serum free cortisol value and lactate level

Treatment
Intensive treatment, potentially to ITU level
Tailored antimicrobials if possible - limited options with viruses
Treatments include: analgesia and antipyretics, physiotherapy, bronchodilators and N-acetylcysteine, suctioning and bronchial hygiene, ventilation
Pathogenesis
Causative agents can enter the lungs through inhalation, aspiration, spread across mucous membrane (some viruses), haematogenous spread (occasionally, e.g. IV drug users with S. aureus septicaemia) and penetrating injury (rare).
Immune response is triggered in the lung and there are local defence factors in the respiratory secretions
Cilia, if functioning, will move material up the respiratory tract, but if damaged this physical defence is impaired
The lungs also have a resident macrophage population (alveolar macrophages) but they are of limited use against several respiratory pathogens that possess a capsule
some organisms can even replicate in these cells
Damage to the lung is caused by the microbes and the immune response
Enzymes released by the bacteria
Factors released by immune cells that cause local irritation and cell apoptosis
Systemic manifestations follow eg
Oxygen deprivation – thickening of the membranes reduces gas transfer
Systemic shock – especially with Gram-negative bacilli such as Haemophilus influenzae


Different anatomy notes form this semester Supplies used (not all at once, I mix and match): Faber-Castell Coloured Pencils (48 Pack) - https://amzn.to/2Kd1mUy Staedtler Triplus Fineliners - http://amzn.to/2pghonI Stabilo Point 88 Fineliner - https://amzn.to/2qU8fC9 Sharpie Pens - https://amzn.to/2HTRmP2 Uni Pin 0.1 Fineliner - https://amzn.to/2HmXp1z Crayola Supertips - https://amzn.to/2HVW1jr Bic Ballpoint Pen - https://amzn.to/2HmCjk0 Stabilo Swing Cool Highlighters - https://amzn.to/2HKxPTu
Influenza
Happy flu season! I’ve just been stuck inside for 5 days with a mild case, so this is a bit bitter
There are 3–5 million cases of flu per year, and ~375,000 deaths, usually in older, younger, and immunocompromised individuals.
Enveloped, Single-stranded RNA virus
First identified in 1933, but existed long before
Generally considered an infection of the bronchi
so effectively a form of bronchitis – i.e. it causes inflammation of the bronchi
There are 3 types - A, B and C
B & C appear restricted to humans
C is less common
A is found in wide range of species including pigs and poultry as well as man
Type A appears to be responsible for more severe disease

Basics
Transmission by aerosols
Incubation ~2 days
Contagious during first 3-5days of illness
Symptoms – fever, myalgia, headache, dry cough, sore throat, aches, fatigue
Recovery ~7-10 days for most
Complications – most frequent = secondary bacterial pneumonia, rarely = viral pneumonia, myocarditis, encephalitis
No specific treatment
Vaccination for high risk groups including the elderly, health care workers, those with underlying respiratory conditions.
Avian
The main reservoir is wildfowl that are resistant to the disease
doesn’t usually affect animals other than poultry and pigs
However some transfer events occur
Seasonal
Incidence highest in winter
Strains vary from year to year - hard to predict and vaccinate (this year’s vaccine has been pretty rubbish)
Pandemic
Can be caused by any strain that has not been seen in the human population for many years
New strains evade the herd immunity that exists to previously encountered strains
1918 /19 –( Spanish) estimated 40-50 million deaths worldwide
1957 – Influenza A/H1N1 (Asian)
1968 – Influenza A/H3N2 (Hong Kong)
Eventually the virus runs out of susceptible hosts and the epidemic fizzles out
Experts generally agree another pandemic is inevitable, and may be imminent – maybe we have had some minor pandemics
16000 confirmed H1N1 deaths in 2009 affecting over 200 countries
Consensus is that the prompt action of the Hong Kong authorities probably prevented a pandemic in 1997
The prediction is scary - for industrialised countries they predic 1.0 – 2.3 million hospitalisations
280,000-650,000 deaths
in two years
A network of 112 centres monitor flu isolates to identify unusual strains that can then be examined further
The WHO has a Pandemic Preparedness Plan in place http://www.who.int/influenza/preparedness/pandemic/en/
Diagnosis
Generally based on GP diagnosis
Virus isolation / virus demonstration from nasopharyngeal secretions during acute phase
Demonstration of viral antigen in secretions
Antibody rise using paired sera ( 1st sample taken between days 1-3 of illness, 2nd taken around day 12 of illness) by haemagglutination inhibition or complement fixation test
Molecular methods evolving rapidly – in particular in response to the recent epidemic/pandemic strains emerging
A range of respiratory illnesses have the same symptoms, only laboratory testing can confirm the aetiological agent
Treatment/Vaccination
In the UK NICE argue that immunisation against predicted strains is the best form of defence – traditionally focused on the elderly and those with underlying lung problems, but recently started rolling out a childhood vaccine (nasal spray)
Vaccines generally based on the H & N surface structures which mutate, however hopes of an M protein based vaccine which will give longer lasting protection raised recently
Antivirals
Antivirals not recommended in otherwise healthy people (amantadine should not be used at all) - should ride it out
However when incidence reaches a certain level zanamivir and oseltamivir should be used in those considered high risk for the development of complications – PROVIDED THAT TREATMENT IS STARTED WITHIN 48 HOURS OF ONSET OF SYMPTOMS
Resistance is becoming an issue

Satellite phenomenon of Haemophilus influenzae around Staphilococcus aureus in blood agar
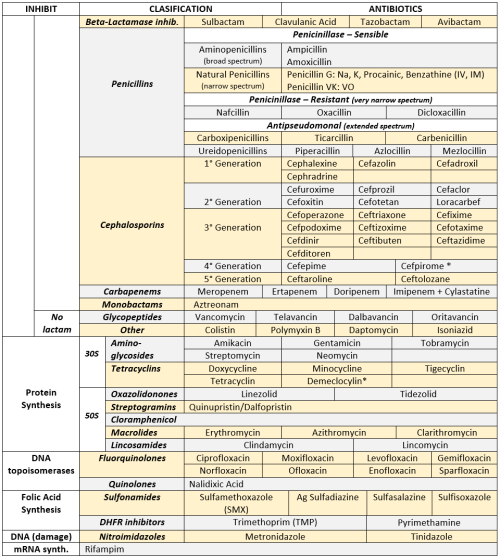
ANTIBIOTICS CHEAT SHEET :)
Also, REMEMBER!!!!
* Sulfonamides compete for albumin with:
Bilirrubin: given in 2°,3°T, high risk or indirect hyperBb and kernicterus in premies
Warfarin: increases toxicity: bleeding
* Beta-lactamase (penicinillase) Suceptible:
Natural Penicillins (G, V, F, K)
Aminopenicillins (Amoxicillin, Ampicillin)
Antipseudomonal Penicillins (Ticarcillin, Piperacillin)
* Beta-lactamase (penicinillase) Resistant:
Oxacillin, Nafcillin, Dicloxacillin
3°G, 4°G Cephalosporins
Carbapenems
Monobactams
Beta-lactamase inhibitors
* Penicillins enhanced with:
Clavulanic acid & Sulbactam (both are suicide inhibitors, they inhibit beta-lactamase)
Aminoglycosides (against enterococcus and psedomonas)
* Aminoglycosides enhanced with Aztreonam
* Penicillins: renal clearance EXCEPT Oxacillin & Nafcillin (bile)
* Cephalosporines: renal clearance EXCEPT Cefoperazone & Cefrtriaxone (bile)
* Both inhibited by Probenecid during tubular secretion.
* 2°G Cephalosporines: none cross BBB except Cefuroxime
* 3°G Cephalosporines: all cross BBB except Cefoperazone bc is highly highly lipid soluble, so is protein bound in plasma, therefore it doesn’t cross BBB.
* Cephalosporines are "LAME“ bc they do not cover this organisms
L isteria monocytogenes
A typicals (Mycoplasma, Chlamydia)
M RSA (except Ceftaroline, 5°G)
E nterococci

* Disulfiram-like effect: Cefotetan & Cefoperazone (mnemonic)
* Cefoperanzone: all the exceptions!!!
All 3°G cephalosporins cross the BBB except Cefoperazone.
All cephalosporins are renal cleared, except Cefoperazone.
Disulfiram-like effect
* Against Pseudomonas:
3°G Cef taz idime (taz taz taz taz)
4°G Cefepime, Cefpirome (not available in the USA)
Antipseudomonal penicillins
Aminoglycosides (synergy with beta-lactams)
Aztreonam (pseudomonal sepsis)
* Covers MRSA: Ceftaroline (rhymes w/ Caroline, Caroline the 5°G Ceph), Vancomycin, Daptomycin, Linezolid, Tigecycline.
* Covers VRSA: Linezolid, Dalfopristin/Quinupristin
* Aminoglycosides: decrease release of ACh in synapse and act as a Neuromuscular blocker, this is why it enhances effects of muscle relaxants.
* DEMECLOCYCLINE: tetracycline that’s not used as an AB, it is used as tx of SIADH to cause Nephrogenic Diabetes Insipidus (inhibits the V2 receptor in collecting ducts)
* Phototoxicity: Q ue S T ion?
Q uinolones
Sulfonamides
T etracyclines

* p450 inhibitors: Cloramphenicol, Macrolides (except Azithromycin), Sulfonamides
* Macrolides SE: Motilin stimulation, QT prolongation, reversible deafness, eosinophilia, cholestatic hepatitis
* Bactericidal: beta-lactams (penicillins, cephalosporins, monobactams, carbapenems), aminoglycosides, fluorquinolones, metronidazole.
* Baceriostatic: tetracyclins, streptogramins, chloramphenicol, lincosamides, oxazolidonones, macrolides, sulfonamides, DHFR inhibitors.
* Pseudomembranous colitis: Ampicillin, Amoxicillin, Clindamycin, Lincomycin.
* QT prolongation: macrolides, sometimes fluoroquinolones
hey! could you do a study tips post on studying w friends who aren't doing the same subjects? like, how to make good flashcards/questions and answers etc so they can quiz you and give you hints etc even if they don't know the content?
How to Effectively Study with Friends
Using Flash Cards
Oh easy peasy! Simply write examination style questions on your flashcards - that way when your friends read the questions out to you, you’ll be testing yourself in a way that might show up on the easier exam questions. Reason being that in order to cover all the topics, your questions will tend to be somewhat simple e.g. describe the different components of x, explaining how they related to y. Obviously, flash cards aren’t the best way to study more complex interrelationships between ideas/concepts, which should be explored more in a mind map fashion. For tips on mind maps, you can check out my briefing here.
Using Your Existing Study Notes
Other than flash cards, if you intend to study in groups for most subjects, one of the best ways to do that is to use the Cornell Notetaking System (which you can read about with my personal tips here). Writing the questions out as you study saves you the trouble of writing out questions for your friends to test you on, and as well as that, means you can test yourself almost as well without them for any times when you’re studying solitary.
Using Essay or Long Response Questions
For long response essays, it’s better to use principles like the rubber duck method, i.e. explaining how concepts relate to each other as if the other person doesn’t know anything about it. So give your friends a list of essay questions and explain part by part in a logical sequential order how you would answer that question e.g. I would talk about the involvement of person A in event B, and explain their impact through examples C, D and E, etc.
Choosing the Right Study Group
Most of all, make sure you rally and encourage each other. Work with people who are like-minded, rotate between each other and have someone who will keep the others on task when you start getting too carried away when studying. Having a goal on what you intend to get finished during a group study session will make sure you always get more out of the session than studying alone!
Hope that helps! ^_^

13.02.18 Revision
I’ve always got my trusty reference book with me at work, but sometimes I like to read over a few topics just in case anything ever shows up :) and oml trying to write referral letter templates be like: …has been measuring … measured between 5-12 mmol/L … BGL measuring between 5-12 mmol/L OTL
🎼 The Boots - Gugudan 구구단
Follow optomstudies for daily original posts and study masterposts! Links: all originals + langblr posts + 15-part college 101 series + web directory!

Hello everyone, welcome to my latest 4-part series to help you land that job after uni! This series will cover what to do before, during, and after a job interview to ensure you leave a positive impression on the interviewers and hopefully help you cinch opportunities! Enjoy!
How To Set Your Career On The Right Path Before You Even Graduate! (Link) Part 2: During The Interview (Link) Part 3: After The Interview (Link)
Research the job position and company values.
It is critical to tackle all the requirements in your cover letter as well as your resume, and to be able to answer questions in the interview in a way that highlights you have those values the company is seeking. Even if the company doesn’t have a public ad, research similar positions at different companies and read those job descriptions. Have situations you’ve dealt with in your arsenal for answering situational questions.
Make sure your resume is updated perfectly.
It’ll save you a lot of time if you just update your resume every time you start something new! Standard stuff: Use ‘clean’ standard fonts, white A4 paper, single sided, 2 cohesive colours max. Include at least the minimum components or a combination of them: the rough order should be:
Career Objective
Education
Relevant Experience (include key responsibilities and noteworthy performance points)
Extra-Curricular Activities (if relevant)
Skills
Referees (usually just write “available on request”)
Cold call!
This is how I got my first relevant job as an optical assistant, which in a way, led to my current position today. Even whilst I was working as an optical assistant, occasionally we would get a new hire if their resume seemed good and they interviewed well.
Prepare for common interview questions.
Have scenarios ready illustrating how you dealt with a difficult situation









nasty moodboard
-
 nicolenoav liked this · 1 year ago
nicolenoav liked this · 1 year ago -
 devinfreetime liked this · 5 years ago
devinfreetime liked this · 5 years ago -
 angelaellar reblogged this · 5 years ago
angelaellar reblogged this · 5 years ago -
usmlereblog4-blog liked this · 6 years ago
-
 bajiraokaushal-blog liked this · 6 years ago
bajiraokaushal-blog liked this · 6 years ago -
 t-b-a-blr-blog reblogged this · 6 years ago
t-b-a-blr-blog reblogged this · 6 years ago -
t-b-a-blr-blog liked this · 6 years ago
-
 superspypeanutjudge-blog liked this · 6 years ago
superspypeanutjudge-blog liked this · 6 years ago -
3rdyearsucks-blog reblogged this · 7 years ago
-
 kariinaa16-blog-blog liked this · 7 years ago
kariinaa16-blog-blog liked this · 7 years ago -
hamzastuff liked this · 8 years ago
-
 paolocabeza-blog liked this · 8 years ago
paolocabeza-blog liked this · 8 years ago -
 bqhhj liked this · 9 years ago
bqhhj liked this · 9 years ago -
 porteblindate liked this · 9 years ago
porteblindate liked this · 9 years ago -
 enarmeandoando liked this · 9 years ago
enarmeandoando liked this · 9 years ago -
 yazz-r liked this · 10 years ago
yazz-r liked this · 10 years ago -
 drhugosavi-blog liked this · 10 years ago
drhugosavi-blog liked this · 10 years ago -
 sedaks liked this · 10 years ago
sedaks liked this · 10 years ago -
 uccikesilaga liked this · 10 years ago
uccikesilaga liked this · 10 years ago -
 diaahamouda liked this · 11 years ago
diaahamouda liked this · 11 years ago -
 usmle1mikmonics reblogged this · 11 years ago
usmle1mikmonics reblogged this · 11 years ago -
 archeroflight liked this · 11 years ago
archeroflight liked this · 11 years ago -
 coeurd-coeurs-blog liked this · 11 years ago
coeurd-coeurs-blog liked this · 11 years ago -
 lady-glam liked this · 11 years ago
lady-glam liked this · 11 years ago -
drpoojakeshri-blog liked this · 11 years ago
-
 missnoemi21 reblogged this · 11 years ago
missnoemi21 reblogged this · 11 years ago -
 schwann86-blog reblogged this · 11 years ago
schwann86-blog reblogged this · 11 years ago -
 misbehavingmyself liked this · 11 years ago
misbehavingmyself liked this · 11 years ago -
 icva reblogged this · 11 years ago
icva reblogged this · 11 years ago -
icva liked this · 11 years ago
-
 amedstu liked this · 11 years ago
amedstu liked this · 11 years ago -
 thecolorsofhope-blog liked this · 11 years ago
thecolorsofhope-blog liked this · 11 years ago -
 ipugmini liked this · 11 years ago
ipugmini liked this · 11 years ago -
 overcomeinsanity reblogged this · 11 years ago
overcomeinsanity reblogged this · 11 years ago -
 yupyaki4life reblogged this · 11 years ago
yupyaki4life reblogged this · 11 years ago -
yupyaki4life liked this · 11 years ago
-
 cherrierenee reblogged this · 11 years ago
cherrierenee reblogged this · 11 years ago -
 nopenothinggoingonhere liked this · 11 years ago
nopenothinggoingonhere liked this · 11 years ago -
 myhellhoundisbiggerthanyours liked this · 11 years ago
myhellhoundisbiggerthanyours liked this · 11 years ago -
 mynotes4usmle reblogged this · 11 years ago
mynotes4usmle reblogged this · 11 years ago -
 rainbowcrayons liked this · 11 years ago
rainbowcrayons liked this · 11 years ago -
 oaklandmellow liked this · 11 years ago
oaklandmellow liked this · 11 years ago
